ISSN: 1705-6411
Volume 11, Number 1 (January, 2014)
Author: Dr. John Iliopoulos
I. Introduction
How might we recover this madness, this insolent freedom that accompanied the birth of photography? (Foucault, 1999: 84)
The first systematic theory and practice of clinical photography were undertaken in the psychiatry of the early nineteenth century (Gilman, 1976: 5). There existed photographic studios inside nineteenth century asylums, and picture taking played a crucial diagnostic and even therapeutic role in psychiatry, far more than in any other medical specialism. In order to explain this historical fact, we shall seek recourse to a method which can foreground the anthropological singularity of the photographic image and its ability to render visible the intrinsically anthropological concepts and ideas of early nineteenth century psychiatry. It is in Baudrillard’s reflections that this method can be found. His theory of photography unsettles the commonsensical assertion that the origins of psychiatric photography can simply be located in the conventional epistemological context of the time. Baudrillard helps us see beyond this linear interpretation which holds that since its birth in the nineteenth century, photography has been the scientific medium of absolute objectivity and the instrument of recognition of illness, supposedly providing scientific validity to psychiatric discourse. On the contrary, we shall argue that proto-psychiatry maintained a fundamental relationship with otherness, therefore Baudrillard’s deep seated adherence to the force of duality and the study of alterity can convincingly show how the value of early psychiatric photography did not lay in the identification or the phenomenological classification of the mentally ill, but in photography’s power to depict the insane as radically other, as inhuman. In fact, it was this duality in the heart of the photographic image which, as we shall show, contributed to the birth of psychiatry as a discipline. It is the same duality which persists beneath the calm positivism and the hegemony of the digital governing psychiatric photography to this day.
II. Baudrillard and the Anthropological Kernel of Photography
In order to grasp the unique anthropological function of photography in its clinical psychiatric setting, we need to follow Baudrillard’s line of reasoning and the way he successively dismantles the misconceptions surrounding the interpretation of the photographic image.
First and foremost, Baudrillard disputes the alleged realism of the photographic image. It is commonplace to take photography as an objective description of the world, a direct evidence of its reality. Baudrillard reverses this assertion. He holds that with photography objects turn into images, pure appearances which, rather than offering a faithful reproduction of reality, place image and reality in strict opposition. The fragmented, instantaneous, discontinuous world of the image, Baudrillard argues, creates another scene, a self-evidence belonging to the order of illusion: ‘the photographic image is the purest, because it does not simulate time or movement and keeps to the most rigorous unrealism’ (Baudrillard, 1999b: 130). The world of photography is a phenomenological world where appearances have ‘gained their independence, are turning around us, turning against us, through the very technology we use to drive them out’ (Ibid.: 129).
This phenomenological world, however, defies the very principles of phenomenology itself. In photography, the object ‘does not want to yield up its meaning.’ (Ibid.: 129). Phenomenology aspires to describe phenomena in a rigorous way, yet it presupposes the universality of meaning, the transcendental subject and the context of primal significations. The phenomenological description of appearances is invested with judgment and intentionality. With photography, Baudrillard points out, this whole process is reversed: by interrupting the flow of significations, by imposing silence to the flow of commentary and interpretation, by subtracting dimensions form the real universe, by removing noise, movement, smell and even colour, the photographic image suspends judgment, meaning and the notion of the real itself (Baudrillard, 2001a: 140). It is therefore a sceptical (Barthes, 2005:200-202) and cynical phenomenology (Baudrillard, 2001a:142, Barthes, 2000: 20), a type of negative theology which, through its apophatic operation, takes phenomenology to its limits, by bracketing intentionality and meaning (Baudrillard, 2001a: 142). This is why, for Baudrillard, photography concerns absence rather than presence. It defies the sovereignty of the subject and the imposition of its will to represent, explain and reduce images to discourse: ‘This is a phenomenology of absence which is usually impossible, because the object is normally occulted by the subject as it might be by an overintense source of light, and the literal function of the image is occulted by the ideological, aesthetic and political dimensions, and by the reference to other images’ (Ibid.: 141). Photography records things in the absence of the subject and at the limits of discourse. It exposes objects, faces, bodies and landscapes in their strangeness and unfamiliarity. Operating at the borders of art, science and philosophy, photography is fundamentally an anthropological enterprise (Baudrillard, 1999b: 139), exploring the limits of the human.
Thus, for Baudrillard, photography contains an indispensable anthropological kernel and is permeated by an ineluctable duality. Photography always seizes the inhuman. ‘Only the inhuman is photogenic,’ as he characteristically puts it (Ibid.: 136). Unlike the realm of concepts and discourse which always seeks meaning, imposes a narrative, forces interpretation and explores identities, photography extracts otherness, reaches the boundaries of meaning and stands at the horizon of sense. In photography it is the object which ‘has done all the work’(Baudrillard, 1997: 30), it is the object which confronts the limits of the human, challenges the pretensions of our rational world and the subject’s will for representation, truth and order. But even when it is not objects but human subjects who are photographed, as in portrait photography, the photographic lens still objectifies them. Photography, in this case, does not seek to be objective, as in offering scientific proof or a structural analysis of the subject photographed, but turns the subject into an object, illustrating the most foreign and inaccessible aspects of her subjectivity:
In the photographic process it’s not a question of considering the world as object, of acting as if it was always there as an object, but of making it become object, in other words, of making it become other, of exhuming the alterity beneath its alleged reality, of making it appear as a kind of basic, disintegrative strange attractor, through its very element, of holding this primitive strange attraction in an image (Ibid.: 30).
Photography overcomes the barrier of identity and recognition, in order to be able to capture alterity. It challenges the misconception that human beings must have their identities revealed behind their ordinary, everyday conventional masks, and instead seeks to unveil their secret mask, their hidden alterity, behind their self-evident identity: ‘For the only interesting thing about a person, or a face, is their radical alterity, and rather than seeking their identity behind appearances, we must try to detect this secret alterity behind their identity’ (Ibid.: 31). Photography is at bottom anthropological and analogical, juxtaposing the real world of humans with their parallel, clandestine existence, revealing ‘the masked divinity which inhabits every one of us, even the most insignificant, for an instant, one day or another’ (Ibid.: 31).
III. Psychiatry as Anthropology
It is precisely at this shared anthropological and analogical level that the common destiny of photography and psychiatry can be analyzed. We shall see how the basic anthropological character of psychiatry in its early years and its formation as an analogy of medical thought, created its close affinity to photographic practice as Baudrillard conceptualizes it. In its birth, the representation of mental disorder escaped both the objectivism and the phenomenological constraints of the medical image and it was the fundamental confrontation with the inhuman which generated the distinct use of photographic images inside the asylum. This is why the photography of the nineteenth century asylum, although marginal with respect to the production of positive psychiatric knowledge, was consistently and systematically evoked for clinical and diagnostic purposes. And the reason for this was that proto-psychiatry, devoid of any conventional medical means of representing illness, was obliged to made use of the inherent quality of portrait photography to depict, not reality or identity, but alterity. As we shall now show, prior to its positivist pretensions, psychiatric diagnosis was centered around the notion of madness, which was a conceptual entity, a form of radical otherness with no empirical support. By necessity, then, the visible representation of madness could only become possible negatively, which is why it required the unique property of photographic medium, as Baudrillard conceives it, in demonstrating precisely what evaded scientific proof, medical discourse, ordinary differential diagnosis and the classical medical representation of illness. Photography constituted an instrument of duality, of a fundamental dual diagnosis between the empirical evidence of illness and the singular, transcendental notion of madness.
In the early nineteenth century, psychiatry lacked the epistemological standards for the use of photography as a means of scientific proof and rigorous clinical demonstration. In the rest of medicine, there was a strictly phenomenological field, a game of portraits, which determined differential diagnosis, that is, the discernment between various illnesses, making up the medical perception of the time in the coupling of ‘a hearing gaze and a speaking gaze,’ as Foucault would put it (Foucault, 2005: 138). Medical perception, however, did not simply constitute a two-dimensional space, a depthless space of differential truth; it was linked to a third dimension, an endoscopic space, which, with the aid of autopsies and microscopic analyses, supplemented diagnostic truth with an empirical and accurate knowledge and the power of objective reality. Thus, in medicine, photographic plates, microscopic illustrations and anatomical sketches provided a wealth of pictorial realism. The newly born psychiatric practice, on the other hand, was permeated by deep internal epistemological problems which prevented such a form of documentation, which is why the realistic depiction of illness in psychiatry was not possible. Whilst there were efforts to use photography as a means of sanctioning proto-psychiatry as a valid scientific method in resolving legal disputes, aiding police surveillance and promoting security techniques (Tagg, 1988: 77-81 and Ellenbogen, 2012), there was no objective truth that would enable the psychiatrist to demonstrate illness microscopically in order to conduct evidence-based forensic analyses, statistical observations and experimental research; that is, to perform the role of a proper clinician. The psychiatrist could not visualize the reality of madness, she could not substantiate its existence and justify its presence scientifically. She could not provide the courts with visual proof in order to ensure medical grounds for restraining the mad and diagnosing them as carriers of risk and danger. Her discourse was not supported by optical evidence that could verify sufficiently whether a patient was in need of involuntary hospitalization, whether she was a malingerer, or that a valid prognosis regarding the future threats that the patient might pose, could be made visible. The lack of visual proof deprived the proto-psychiatrist of demonstrative truth, as it was still impossible to pin mental illness to the interior of he body.
Thus, there was only a formal isomorphism and a phenomenological equivalence between proto-psychiatry and the rest of medicine. It was not gnosis or prognosis but solely diagnosis which established an analogon with medical practice (Foucault, 2003: 161). This analogon established formal similarities with the diagnostic truth of medicine, without continuity with the content of medical knowledge. Medical perception in the early years of psychiatry was still a two-dimensional space and diagnosis remained a strictly phenomenological approach to mental disorder, free form theories and speculations. This is why the visual mode of representation of the time consisted mainly of the physiognomic sketches used by the empiricism of the French psychiatric school of Pinel and J. D Esquirol (Gilman, 1982: 72-101). With these illustrations, the proto-psychiatrists ensured a degree of empirical proof of psychiatric symptomatology in order to construct a reliable taxonomy and classification, and an elementary method of transmitting clinical knowledge. Proto-psychiatry remained a medicine of surfaces and appearances. It was a phenomenological discipline, a science of portraits.
Even this phenomenological approach, however, could not cover the entire field of proto-psychiatric discourse and representation. It was the position of madness as radical alterity in the heart of the diagnostic system of early nineteenth century psychiatry, evident both in the theoretical edifice of alienism and in its everyday practice, which precluded the use of rigorous medical knowledge in the study of mental disorder. Whereas in medicine diagnosis was able to cover the entire field of diseases, providing differential knowledge, in psychiatry an absolute diagnosis prevailed, between madness and non-madness. This dualism was indispensable for psychiatric discourse: on the one hand the immanence of everyday clinical perception identifying illnesses and on the other the transcendence of madness which was considered a limit experience conceived by reason as its contrary, its outside, laying beyond the limits of rational comprehension (Foucault, 2006b: 133-134). Madness was not an ordinary medical ailment; it was an inexplicable mental condition beyond the boundaries of the law, the borders of human rationality and the principle of reality. It was ‘deduced and not perceived’, as Foucault would say (Foucault, 2006a: 185), being de jure impossible to identify it in clinical terms and represent it visually, although it could be logically deduced as a real but alien experience which necessitated the involuntary incarceration of individuals and the medical treatment of motiveless criminals. Madness was an elusive but fundamental psychiatric concept, a philosophical idea which, in accordance with Kant’s anthropological project, conditioned the very construction of scientifically acceptable psychiatric discourse, becoming the medical prototype of radical alterity, the inhuman experience par excellence. This experience could not be represented, yet its portrayal was necessary if psychiatry were to acquire the validity of a medical specialism.
This is where Baudrillard’s theory of photography becomes most pertinent. We are now in a position to see how Baudrillard’s reflections can explain why the rudimentary psychiatric knowledge of the early nineteenth century did not hinder the use of photography in a clinical setting, but, on the contrary, constituted the fertile ground for its birth and development. Seen from a Baudrillardean angle, it was exactly the formal isomorphism of psychiatry with medicine, its lack of evidence-based research and its anthropological character which made possible the extensive use of photography inside the asylums. As Baudrillard can help show, it was not photography’s scientific worth which brought about a more accurate representation of the mad; it was not the phenomenological or aesthetic value of photography which supposedly came to substitute for proto-psychiatry’s lack of scientificity. The power of the photographic image to illustrate the inhuman, responded exactly to the paradoxical proto-psychiatric need to study medically an irrational experience in terms of rational descriptions, when all methods of demonstration, medical proof and documentation had failed. Photography, beyond any other artistic or scientific method, was the best tool for picturing alterity, playing an instrumental role in the production of scientific knowledge concerning the insane, and in the construction of the psychiatric subject.
IV. A Baudrillardean Psychiatric Photographer: The Case of Hugh Diamond
Photography emerged in a clinical setting as a radical break with all existing modes of visual representation. There had already been a long-standing tradition in the portrayal of madness, from Bruegel, Hieronymus Bosch, and Munch, up to the physiognomic sketches of Pinel and Esquirol, mentioned above (De Sirvy & Meyer, 1998). All these efforts to visualize madness could masterfully illustrate the world of unreason, but they always contained the language of the painter. While they artfully represented the overflowing passions, the excessive presence of fear, anguish, anxiety or depression of the patients, they were inevitably permeated by elements of exaggeration, graphic description and subjective interpretation. Madness, on the other hand, emerged as a problem for the doctors of the early nineteenth century precisely on account of its lack of expressionism, its meaninglessness, its absurdity and its resistance to any causal or psychological explanations. For the proto-psychiatrists it was not the extravagance of the patient’s passions, but the lack of consciousness that the patient had of them, which determined the need for compulsory admission into an asylum. It was not the overt and clear manifestation of disturbed emotions but their complete absence in the course of murderous acts, which constituted the chief criterion for the medico-legal definition of insanity (Castel, 1988: 142-149). This is why, apart from their general nosographic role, paintings and drawings were of limited clinical value in the early nineteenth century asylum; whilst portraying human suffering with the greatest aesthetic skill, they failed to capture the patients’ underlying delirium which resists the most skilful naturalism. British neurologist Sir Charles Bell had already highlighted the limitation of the arts to go to this absent heart of alterity: ‘The error into which a painter would naturally fall, is to represent this expression by the swelling features of passion and the frowning eyebrow; but this would only convey the idea of passion, not of madness’(Bell, 1806: 155). Thus, a new mode of representation was needed, a more abstract and irreal visual technique which, as John Conolly, one of the major reformers of the British asylum, observed, would surpass the traditional, realistic means of representing ‘the ordinary expression of the passions and the emotions,’ portraying instead the critical, singular moment when ‘reason is beginning to remit its control,’ and ‘wits are just beginning to wander away from the truthful recognition of things’ (Gilman, 1982: 167).
With the advent of photography, this extra diagnostic dimension was added. Photography could go beyond the moral, metaphysical or physiological prejudices of painting, imposing the silence of the picture and its direct depiction of a hidden transcendence. It was Hugh Welch Diamond, a clinical psychiatrist who, as resident superintendent of the Female Department of the Surrey County Lunatic Asylum since 1848, made the first systematic use of photography in his clinic, precisely on account of its unique ability to illustrate the alterity of his patients’ experiences, free from the constraints of expressionism, meaningful contexts and dramatic representations of painting, and ‘the painful caricaturing which so disfigures almost all the published portraits of the Insane’ (Gilman, 1976: 24). Diamond thought that the analogical nature of photography, could, more than ‘any laboured description’ (Ibid.: 20) bring forth with the greatest simplicity and maximal abstraction, the aura, the mystery which comes from the patient’s soul to resist the visible order. It is this invisibility, he argues, this elusive essence of the deranged mind, which photography manages to capture: ‘the Photographer catches in a moment the permanent cloud, or the passing storm or sunshine of the soul, and this enables the metaphysician to witness and trace out the connection between the visible and the invisible in one important branch of his researches into the Philosophy of the human mind’ (Ibid.: 20). Hugh Diamond took advantage of photography’s quality to arrest the strangest, most singular details of his subjects. He made use of photography’s ability to defy, as Baudrillard points out, ‘painting… which inevitably strive(s), thanks to a concept, a vision or an internal movement, to limn the figure of a totality’(Baudrillard, 2002: 155).Whereas in painting madness had always been depicted either in its wretchedness (Hogarth), its bestiality (Goya) or its monstrosity (Gericault) (Virilio,1994: 37-39), Diamond’s photographs, were austere, expressionless and immobile. They sought the absence in the heart of the image, without embellishment or pictorial rhetoric. Instead of depicting the wild passions or the danger of the patients’ frenzy, they displayed their inner truth, their private world inaccessible to psychological interpretation. Using the stillness and mute inertia of the photographic image, they explored madness as absence, ‘even in bodies and faces laden with emotion, with pathos’ (Baudrillard, 2002: 152). The patients in these photos emitted the same air of death and savagery as those family photographs and the images of savages in the early years of photography, when the subjects photographed, whether bourgeois or peasants, had the ‘same wild, deathly seriousness as a primitive. Their being is immobilized, their eyes dilated before the image; they spontaneously take on the stature of dead men.’ (Baudrillard, 1999b: 138).
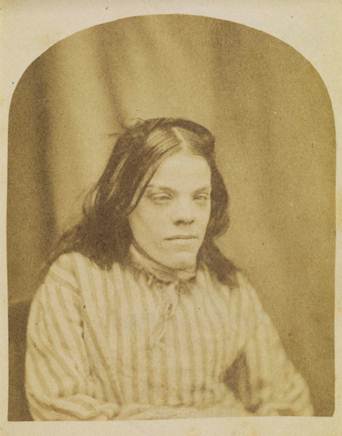
Plate 1
What Hugh Diamond’s photographs explored was not the familiarity with the patients’ emotions, their suffering or their misery; on the contrary, they manifested their secret absence from themselves and the world. In Hugh Diamond’s photographs the patients posed like they wanted to be photographed, looking absent from their own lives and their misfortunes, and it was their destiny which was revealed (Baudrillard, 2002: 151, 2001a: 146).

Plate 2
This is why their long exposure to the lens, their expressionless faces and the absence of background, did not merely add an aesthetic value to these images, as Sander Gildman argues (Gilman, 1976: 8), but enhanced the feeling of estrangement that they emanated.

Plate 3
The patients were isolated from their milieu, they posed willingly but without collusion with the lens. On the contrary, their gaze penetrated the lens, looking into the void, creating a duel with the photographic apparatus (Baudrillard, 2002:151-152).
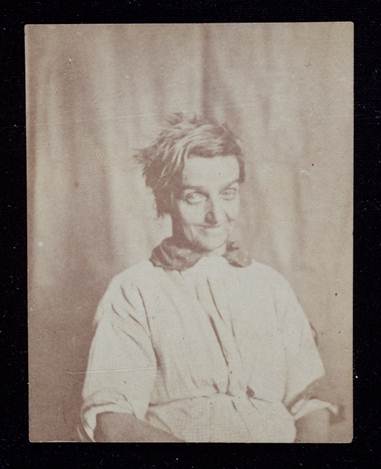
Plate 4
The patients’ photographs did not constitute part of a larger narrative about their diagnosis; they were not merely a pictorial element in the broader discourse about their illness. It was the photograph itself which ‘create(d) the event’(Baudrillard, 2001b: 95), foregrounding the moment of crisis which had occurred in the patients’ lives, the kairos of the emergence of their illness as a singular, unprecedented event of destiny, breaking with all prior causality. In fact, it was by virtue of displaying madness qua rupture with the patients’ ‘normal’ state that the photograph introduced a break with all medical knowledge and known psychology, a break which Hugh Diamond himself used as both a diagnostic and a therapeutic tool: first, by portraying the physical and mental alienation of his patients, he managed to illustrate that madness was precisely that sudden, unexpected and inexplicable experience, irreducible to theories of pathology. His photographs depicted phases of transition from sadness to excitement, from joy and happiness to melancholy and loss of energy (Gilman, 1976: 55, 63). They stood in contrast to the patients’ personal histories to demonstrate the sudden rupture with their previous life patterns, their personality and their ordinary behaviour. In these photographs the patients did not look self-regarding, well-versed in their subjecthood; they were withdrawn and indifferent. They showed no awareness of the events taking place in their lives. No self-consciousness or introspection is at work; this is why their photographs managed so well to capture ‘a gleam of ingenuity, of fatality, in their faces, betraying the fact they do not know who they are or how they live’ (Baudrillard, 2002: 152).

Plate 5

Plate 6
They captured the instant, the moment of crisis when madness bursts forth into the world of appearances to suspend medical judgment, undermining with its silence the ‘thunderous context’ of medical discourse, and imposing its singularity of the instant of its appearance ‘outside of its interpretative context, at the point where things have no meaning or, do not yet have meaning… but appear all the same’ (Baudrillard, 1997: 31). The singularity of these photographs consisted of standing out among all other images and eliminating them, introducing discontinuity into medical diagnostic thinking (Baudrillard, 1999b:146). It was this singularity which Hugh Diamond used in order to bring about the effect of a remedy on his patients: by showing the photographic event to his patients, Hugh Diamond created an effect of derealization; faced with her photographic portrait right after her recovery, the patient was forced to witness the reality and the delusional truth in which she had been trapped during the course of the illness (Gilman, 1993: 353-359, Burrows & Schumacher, 1990: 42). Through this heautoscopy, the patient was challenged to reconsider her own self-evident world and her private reality principle (Barthes, 2000:12-13).
Thus, with its function as a site of dual diagnostic truth, the new technological invention served as the medium for the reciprocal construction of the psychiatric subject and its correspondent object of madness, marking the beginning of psychiatry as a discipline. The conception of photography by the proto-psychiatrists, not as a faithful representation of reality, but as an ‘invocation of the other’ (Baudrillard, 1999a:1), brought this other center stage, as the elusive object of medical representation. Established medical categories could not accommodate the photographed other. On the contrary, it was the other who refused, from deep within her silence, to provide the medical subject with clear and definite answers. Confronted with this enigmatic appearance of the inhuman, of the irrational, the medical subject could no longer ask the photographed other ‘Reply to my questions,’ but ‘Tell me what questions I am to ask you’ (Ibid.: 2), tell me what medical categories I am to impose on you, which methods of treatment I am to apply to your mind and body, in which places I am to confine you and isolate you from society. From the moment when the doctor found herself in the position to pose these original questions to the other, the anthropological problematic was introduced within medical thinking, the proto-psychiatrist as a medical subject was created, and psychiatry was born as a desire for the other and as a response to a fundamental anthropological division.
V. The Digital Revolution
Since the middle of the nineteenth century, psychiatry lost this essential relationship with anthropology. There was a consistent effort to represent the psychiatrist as a stable and timeless subject of mental medicine, and to transform the duality of psychiatric diagnosis and its analogy with the rest of medicine, into a discourse continuous with that concerning somatic disorders. The desire for such continuity necessitated the elimination of madness and its incorporation into the hegemony of positive knowledge. Madness ceased to exist as radical otherness and was abolished as an anthropological concept. Insanity became one illness among others, it became one element in the vast interplay of diseases, one abnormality in the endless proliferation of differential diagnosis. This new differential logic replaced the dualism of the previous period (Baudrillard, 2007:76). It was a logic which prevailed not only in diagnostic discourse, but also in patient imaging. The clinical description of illnesses referred to a binary logic of 0 and 1, to a matrix of alternations, an endless field of genetic or neuroanatomical abnormalities and, at the same time, the pictorial representation of diseases abolished the scene of the body and the surface, it ceased to represent madness by allusion at the level of appearances, and attempted to reduce it to a set of microscopically and electronically visible biological processes. This digital revolution brought about the hegemony of a binary logic which eventually deprived psychiatry of its relationship with alterity: it was not only philosophy and psychology which ‘died at the same moment as ‘the other’, and the desire for the other, died’ (Baudrillard, 1990a:8), but photography also died insofar as it also lost its anthropological dimension, its power of the negative, gradually entering the digital era.
The origins of this historical mutation can be located in the middle of the nineteenth century. Neurology dominated psychiatric discourse, seeking to incorporate the clinical picture and aetiology of madness into the models of automatism and degeneration. A continuum was established between the most irrational manifestations of psychotic patients and the commonest neurotic or erratic types of behavior. This continuum was grounded on a neurological disturbance, supposedly underlying all abnormal behavior, from the monstrous criminal to the everyday pervert. Photography followed the same principle. In Europe, the photographs of the French neurologist Duchenne de Boulogne isolated the facial expressions through localized electrical stimulation, in order to demonstrate the evolutionary and neurophysiological basis of all abnormal behavior, irrespective of its degree of its irrationality (Marles, 1992). Similarly, Cesare Lombroso criminologist and physician, founder of the Italian School of Positivist Criminology, photographed various criminals in order to establish typical neurological and other anatomical markers of degeneration that could be linked to potentially dangerous behavior associated with mental disorder. His photographs, along with his anthropometric studies, inserted a political dimension into psychiatric discourse, turning psychiatry into a political force of discrimination between genuine political reform and sterile violence due to mental illness. By illustrating the physical defects in the physiognomy of anarchists, Lombroso sought to introduce biological, physiological and anatomical criteria for the distinction between insane deviants and authentic revolutionaries, conducting a type of anthropology laden with racist overtones (Horn, 2003: 16-25).
Likewise, the early American psychiatric photography of the nineteenth century echoed the efforts to reclassify madness as an organic disease, seeking to minimize the differentiation between normality and abnormality, rather than accentuate it. Dr. Thomas Story Kirkbride, a neurologist at the Pennsylvania Hospital for the Insane, used the ‘magic lantern’, slide shows, much like the slide projectors used today, as a type of neurophysiological therapy whereby patients could integrate rational thinking into their disturbed perception (Layne, 1981 and Godbey, 2000: 31-69). Instead of photographing the patients themselves, Kirkbride’s ‘magic lantern’ displayed pictures of the outdoor environment in order to educate and train the patients for the outside world (Godbey, 2000: 39). Instead of derealizing the patients’ mental state, his photographs intensified and reinforced the reality principle which was supposed to act as a force of treatment and therapy. Contrary to Diamond’s effort to single out the strangeness and foreignness of insanity with respect to the world of reason, the aim of Kirkbride’s photographs was to reduce the gap between madness and sanity so as to aid the patients in acquiring a sense of normality (Ibid.: 50). The ideal end goal was to make the patient adjust to the environment, rather than to illustrate her alienated world. Moreover, these photographs supposedly had a direct biological and therapeutic impact on the patient. Following the assumption that the light emitted from lens could reach the brain, bringing about a direct physical alteration on the patient’s cerebral chemistry, photography became not only a technical medium of representation, but also a biochemical tool, an instrument with the capacity to modify brain structure (Ibid.: 54-57).
This new medical role of photography represented the initial episode in the new conception of patient imaging and its ability to yield the truth about madness. The photographic representation of mental illness became more sophisticated over the years, offering more accurate modes of imaging, with the addition of color, movement, instantaneity and 3D projections. Clinical photography became orientated towards documentation and reportage, providing direct representations of the illness itself, without the mediation of discourse. The ideal end goal was no longer to offer a freeze frame of the patient at the level of appearances, but to extract a more ‘realistic’, cinematic illustration of the bodily depth of madness, down to its molecular level. To this day, the photographic image has become an anthropometric study of the mentally ill, similar to Lombroso’s studies; it has increased the level of pictorial abstraction in order to reveal the most elementary neuroanatomical matrix of insanity. Moreover, it is now manipulated digitally so as to interact, like Kirkbride’s photographs, with the nervous system, in order to alter its functioning, and extract its ontological truth. In light of these transformations, contemporary psychiatric photography is no longer anthropological, not even phenomenological; it is ‘speleological […] (the) videoscopy of the inside of the body by micro-cameras, a cleft opened into the abyss of the entire body’ (Baudrillard, 2005a: 194). Current images have become endoscopic, penetrating the surface of the body and, free from diagnostic truth, aim to ground that truth on the transparency of the reality of disease.
This is especially the case with digital techniques of brain imaging. It is no longer the face, the body, the gestures of the patients that may hold a diagnostic secret. The secret of the illness is considered to lie in the brain, which, as the foundation of every mental disorder, interacts with the digital camera which projects brain activity on a screen. In fMRIs, SPECT and PET digital scans, it is the screen which kills off the image as analogon (Baudrillard, 2009:45). These digital scans do not offer one image which eliminates all the others by foregrounding the transcendental idea of madness ‘capable of being imagined’ (Ibid.: 45). They provide, on the contrary, an infinite reproduction of calculations and an endless ‘proliferation of images’ (Ibid.: 40). There is only an abstract referent in these images, a simulation of brain activity which destroys any ‘classification or signification, any modality of meaning’ (Baudrillard, 1981: 108), insofar as the screen bypasses the distance of the mirror of taxonomy, it absorbs diagnostic truth and strives to represent the reality of illness in the real time of synaptic interactions. But it is ‘totally wrong-headed’, Baudrillard points out, ‘to see the brain as a receiver, a screen for brain images in real time’ (Baudrillard, 2009:43). Such a reduction of human intelligence to a ‘miniaturized terminal’ (Baudrillard, 1993: 48), this condensation of the mind in the circuits of the brain which interface with the machine according to a single program, renders the rest of the body useless (Ibid.: 48). It abolishes the face, and thus fails to suggest otherness, not because it misses the facial expression of the soul, but, on the contrary, because it fails to bring forth the ‘absence of the subject reinforced by every feature of a face’ (Baudrillard, 1996: 86). It abolishes the gaze, the duel signs of the eyes, which, without depth or temporality, sum up ‘the body’s full potential (and that of its desires?) in a single, subtle instant, as in a stroke of wit’ (Baudrillard, 1990b: 77). It abolishes the body as a source of traps, illusions, sexuality, pleasures and suffering: ‘No more faces, no glances, no human figures or bodies there — organs without bodies, flows, molecules, fractals’(Baudrillard, 2005a: 92). Digital photography follows the model of the disembodied patient and employs the notion of the abnormal individual who is no longer other, living ‘only in a unilateral positive adherence to what he is and what he does. Total subjection and adjustment (the perfectly normalized being)’ (Baudrillard, 2009:68).
VI. The Anthropological Revolution
The digital revolution, however, is not the last word of the image. There is an evil demon hiding inside images, a property of the photographic image turning against the model of integral reality, programming and manipulation. In the heart of the hegemony of the digital which promotes the incessant flow of images, disregarding any contradiction, blanks or negativity, the image reinstates the negative, the ‘freeze’ and the duality in the heart of representation. It reintroduces the parallel world of evil, negativity and the inhuman. It brings about the anthropological revolution inside psychiatric representation, a revolution ‘exactly antithetical to our current digital ‘revolution’’ (Ibid.: 64).
Madness destabilizes the abstraction, genetic manipulation and hyperreality of psychiatric practice, it inserts the irreconcilability of its otherness, its exceptionality and its singularity, and photography is there to record that otherness negatively. Only photography can illustrate without mediation those instances when madness defies the dialectical principle of psychiatric discourse. It is the power of the photographic image to undermine the medical model which encompasses all negativity, and to subvert the humanitarianism and the moral anthropology of current psychiatric practice which nowadays exists ‘to reconcile the irreconcilable’(Ibid.: 67-68). Only photography, with its objective irony, can challenge the three-dimensional world of moral representation, psychological meaning and cultural homogenization, becoming madness’ tool of evasion and illusion. It is the photographic medium, ‘diabolical and perverse’, which leaves the question of madness ‘eternally in suspense, but also eternally thwarts human undertakings (all based on synthesis, integrality and the deliberate forgetting of all refractory forms, of everything that cannot or will not be integrated or reconciled…)’(Ibid.: 67).
Thus, since the nineteenth century, photography has reproblematized the intrinsic duality of diagnostic truth, free from the obsessive concern with the ontological reality of mental illness. Photographs taken by doctors, patients and non-professionals in the field of mental health, have challenged the clarity of psychiatric positivism, raising diagnostic problems of anthropological nature. Crucially, they have recorded the consistent resistance of the body to the institutional power of psychiatry, not by recording the supposed naturalness of the body against its artificial manipulation by clinical discourse, but on the contrary, by staging the body’s theatricality, its primitivism and its hidden pleasures, which defy its narrow neurological and neuroanatomical definitions. Anthropologically inspired photographs turn the body of the insane into an image behind which insanity itself enacts its own disappearance, leaving only its traces available to the medical gaze (Ibid.: 32)
This was the case with the photographic depiction of hysteria in the nineteenth century. Jean Marie Charcot made extensive use of the Salpetriere photographic studio in order to capture the versatility of the hysterical symptomatology (Didi-Huberman, 2003:29-66). Aspiring to offer a neurological account of madness, he sought to immobilize the numerous fits, conversions, postures and gestures of the hysterics, using the photographic image as a ‘skillful mirror, like Perseus’ shield, in which Medusa found herself petrified’ (Baudrillard, 1990b: 105-106) that would stabilize the clinical picture of hysteria as proof of its autonomous existence as a clinical entity, free from the suspicion of simulation. However, as a combination of ‘the passion of seduction with that of simulation’ (Ibid.: 119), hysteria presented as an appearance without depth, without ontological substrate. The perfectly theatrical, dramatic and immobile image of the hysterical body contradicted the clarity of neurological diagnostic discourse, as no concrete organic reality lay beneath the apparent regularity and stability of the hysterical outbursts. The photographic images of the hysterics created a tension, a Magrittean contradiction between the diagnostic text which only superficially coincided with the clinical picture of hysteria (‘This photo is not a photo’), and the photograph itself which conformed faithfully to neurological diagnosis at the level of appearances, without verifying it anatomically (‘This text is not a message.’) (Baudrillard, 1991:135). The result was a surreal photographic effect, a scene where the madness of hysteria staged its own dramatic disappearance. The photographic image was the prefect medium for this violent absence, a mode of representation which at once sanctioned neurological diagnosis and made it unacceptable. In the case of hysteria, photography aided Charcot’s efforts to offer a neurological model for the explanation of madness, but at the same time, by undermining that model, it became the protagonist in one of the most important reversals in the history of psychiatry, a moment when the will to medicalize insanity was suspended, and has become problematic ever since.
A similar reversal, for the opposite reasons, took place in De Clerambault’s early twentieth century photographs. De Clerambault, a famous French Psychiatrist, travelled to Morocco where he took thousands of photographs of local peasants, all veiled. De Clerambault was one of the leading figures of early twentieth century psychiatry who renewed the question of alienism in the heart of positivist psychiatry, reinstating the notion of madness as radical alterity, which he tried to link to pleasure. He thus theorized insanity as an alien experience associated with a state of mental automatism and an impossible jouissance (Foucault, 2003: 311). By photographing the Moroccan villagers he conducted a unique clinical and ethnological analysis connecting a culture foreign to his own with an inaccessible pleasure. De Clerambault tried to depict the veil both as an everyday cloth and as a cultural and religious accessory to the body, alien to western conceptions of fashion and beauty. Psychoanalytically orientated thinkers argue that De Clerambault’s large number of photographs on the subject betrays his own obsession with the issue of drapery or that it represents a study of a culture’s fetishism and its hidden pleasures foreign to the mere usefulness of clothing by western utilitarianism (Copjec, 1995: 65-116). In a more Baudrillardian vein it can also be considered as an attempt to display exactly the opposite: a ‘non-fetishist culture (one that does not fetishize nudity as objective truth),’a culture in which the veil ‘abolishes the body ‘as such’’ (Baudrillard, 1990b: 33). De Clerambault portrays a culture of the veil in which what is challenged is precisely the transparency of the body which ‘appear(s) as definitely enigmatic, definitively secret, as a pure object whose secret will never be lifted and has no need to be lifted’ (Baudrillard, 2005a: 186). De Clerambault makes no effort to look for bodily signs of degeneration, the way Lombroso does. His photographs do not analyze physiognomy and do not conduct anthropometry. On the contrary, they challenge the notion that a medical knowledge of the naked body is necessary in order to reveal the other’s truth. In a symmetrical but opposite way to hysteria where the naked body offers ‘booby-trapped’ signs that confuse medical discourse (Baudrillard, 1990b:119), the veil stands itself as the sign that tears the body of ‘its nudity, naturalness and ‘truth’, from the integral reality of physical being’ (Baudrillard, 2005a: 186). This is why De Clerambault’s obsessive depiction of the veil contributes nothing to the positivist history of psychiatry; on the contrary, it suspends full knowledge of the other, enacting the Nietzschean motto that ‘we no longer believe that the truth remains truth once the veil has been lifted’ (Baudrillard, 1990b: 59). Unlike those photographs taken in a positivist context aspiring to elicit pre-conceived answers from the subject, it is Clerambault’s photography which determines which questions, whether psychiatric or ethnological, are to be posed to the photographed subject. They create the necessary distance between the subject and the object to allow truth to emerge, rather than impose a pre-determined meaning. This is why Baudrillard reacted in a De Clerambaultian way, when, 80 years later, this forced signification took place in the Abu Graib photographs and the violent unveiling of the Arab prisoners. Baudrillard posed the crucial clinical and anthropological question: ‘what does one want these men to acknowledge? What is the secret one wants to extort from them? […] Radical shamelessness, the dishonor of nudity, the tearing of any veil. It is always the same problem of transparency: to tear off the veil of women or abuse men to make them appear more naked, more obscene…’(Baudrillard, 2005a: 209).
The same radicalism of the image, the same split inside diagnostic discourse, emerges when the patients themselves perform the photographic act. In Impossible Exchange, Baudrillard discusses the case of David Nebreda, a Spanish photographer with a diagnosis of schizophrenia who, in his Autoportraits, photographed himself in a state of extreme emaciation, destitution and complete isolation. While the commonsensical approach would be to argue that Nebreda’s photographs document and confirm the clinical manifestation of his mental illness … Nebreda exhibits his lacerated body caused by multiple self-injuries, there are bodily signs of self-neglect and deprivation due to the chronicity of his schizophrenia … Baudrillard singles out those aspects of Nebreda’s photography which escape the context of mere documentation. First and foremost, while Nebreda’s social withdrawal, cognitive impairment and sensory deprivation should normally preclude the possibility of any creative act … Foucault’s notion of madness as the ‘absence of an oeuvre’(Foucault, 2006a: 541-549)… his photographs are elaborate pieces of artistic creation, even in its extreme form: ‘Confined in a single room, seriously ill, he unflaggingly photographs his own torment, his own tormented body, varying the décor, the lighting and the staging of a dead-end worldd… He manages to deny himself absolutely and to produce that denial as work, and even as artwork. For his photos are not a mere testimony, they are works’ (Baudrillard, 2001a: 125-126). As part of these works, Nebreda exposes his own body, not as an act of self-pity, or with the intention to provoke sympathy for his suffering or antipathy towards the psychiatric establishment. His photographs do not simply record his mental condition as scientific proof of his illness, nor do they turn it into an artistic spectacle or an advertising act. Nebreda’s body appears as an object which, in an act of mockery, identifies with the signs that are inscribed in it. Unlike hysteria where the body turns into a sign to undermine the orthodoxy of neurological symptomatology, in Nebreda it is the signs of his illness which become living, real, material and physical: ‘he finds the strength to inscribe himself in a living sign, the living equivalent of that mental destruction — the sign of his own body’(Ibid.: 126). In an untitled image, Nebreda’s naked body is surrounded by four sheets, pasted onto a black background, in which a text writes: “David Nebreda de Nicolas: born 1st August 1952; chronic paranoid schizophrenia; he follows the order; today 19th October 1997. D.N.N. He does it; with his excrement. Against vertigo, nothing can be said’ (Jones, 2005:5-6). In this photo, Nebreda not only parodies the conventionality of his diagnosis as a schizophrenic, but uses his own body as a living statue of the medical truth which permeates him. In fact, this very medical truth, his diagnosis, is written in his own excrement, creating a mockery of his psychiatric profile, transforming the signs that purport to represent his illness into a literal extension of his suffering body. Thus, Nebreda questions the existential notion of his embodied subjectivity by turning his body into an object and a spectacle, whereby he confuses his own lived experience with the representation of that experience. He is sane enough to be able to represent his condition with carefully worked out images, but insane enough to use the sacrifice of his own body as a means of turning medical significations against themselves. In fact, this is precisely where the artistic aspect of his mad work lies: ‘Art is made from the impossible exchange of signifier and signified, and therefore from the impossibility of representation as such, which is made up of dead signs and empty promises’ (Baudrillard, 2001: 126).
VII. Conclusion
Photography introduces a model of analogical thought. ‘This is more or less the object of analysis: to get closer to the analogical heart of the event and thought’ (Baudrillard, 2010: 35). By unsettling the principle of reality, representation and objectivity, photography introduces a critical distance between words and things, between subject and object, truth and reality (Baudrillard, 2005b: 96); it inserts the two-dimensional scene of illusion and negativity into the heart of the digital world of numerical calculation and virtual reality. The value of the analogical image for psychiatry, in particular, consists of reinstating the anthropological root of psychiatric epistemology inside the medical integrism which incorporates the radical alterity of the inhuman into the universe of positivism. Medical rationality imposes a continuous, metonymic discourse which aspires to establish an epistemological equivalence with psychiatry in order to reify madness as a form of illness. By contrast, the exceptional, singular photographs analysed in this essay, foreground the metaphorical, analogical isomorphism between psychiatry and the rest of medicine, as well as with other disciplines. By staging madness as an object that can be contemplated anthropologically but not represented scientifically, photography demarcates the limits of psychiatric positivism, generating an interdisciplinary field where science, philosophy, art, ethnology and psychoanalysis can operate as legitimate grids of anthropological analysis. It is in the neutral space of photography, in the silence and the inertia of the image which interrupts the endless proliferation of discourse and interpretation, that these heterogeneous disciplines can interact, come into conflict and question each other. This is why, as Baudrillard would put it, after the anthropological challenge brought about by photography, ‘how can you go on doing your own thing in your own little discipline as though nothing had happened?’ (Baudrillard, 2004:56).
About the Author
Dr. John Iliopoulos is from the Hellenic Air Force Hospital, Athens, Greece.
References
Roland Barthes (2000). Camera Lucida: Reflections on Photography. London: Penguin.
Roland Barthes (2005). The Neutral: lecture course at the College de France, 1977-1978. New York: Columbia University Press.
Jean Baudrillard (1981). Simulacra and Simulation. Ann Arbor: The University of Michigan Press.
Jean Baudrillard (1990a). Cool Memories (1980-1985). New York: Verso.
Jean Baudrillard (1990b). Seduction. New York: St. Martin’s.
Jean Baudrillard (1991). ‘Barbara Kruger,’in Gary Genosko. The Uncollected Baudrillard. Thousand Oaks, CA: Sage.
Jean Baudrillard(1993). Baudrillard Live. London: Routledge.
Jean Baudrillard (1996). The Perfect Crime. London: Verso.
Nicholas Zurbrugg (Ed.). (1997). Jean Baudrillard: Art and Artefact. London: Sage Publications.
Jean Baudrillard and Luc Delahaye (1999a). L’Autre. London: Phaidon Press.
Jean Baudrillard (1999b). Photographies (1985-1998) Ostfildern-Ruit, Germany: Cantz..
Jean Baudrillard (2001a). Impossible Exchange. London: Verso.(Nebreda).
Jean Baudrillard (2001b). ‘Notes on the Impossible Exchange.’ In The Gift. Edizioni Charta, Milano.
Jean Baudrillard (2002). The Transparency of Evil. London and New York: Verso.
Jean Baudrillard (2004). Fragments. London: Routledge.
Jean Baudrillard (2005a). The Conspiracy of Art. New York: Semiotext(e) / MIT.
Jean Baudrilllard (2005b). The Intelligence of Evil or the Lucidity Pact. New York: Berg Press.
Jean Baudrillard (2007). Exiles from Dialogue. Polity Press.
Jean Baudrillard (2009). Why Hasn’t Everything Already Disappeared? Seagull Books (London, New York, Calcutta).
Jean Baudrillard (2010).Carnival and Cannibal. New York: Seagull Books.
Sir Charles Bell (1806). Essays on the Anatomy of Expression in Painting. London: Longmans.
Adrienne Burrows & Iwan Schumacher (1990). Portraits of the Insane: the Case of Hugh Diamond. London and New York: Quartet Books.
Robert Castel (1988). The Regulation of Madness: the origins of incarceration in France. Berkeley: University of California Press.
Joan Copjec (1995). Read My Desire: Lacan against the Historicists. Massachusetts: Massachusetts Institute of Technology.
Sophie De Sivry & Philippe Meyer (1998). Art and Madness. Paris: Éditions Du Sextant Bieu.
Georges Didi-Huberman (2003). Invention of Hysteria.Charcot and the Photographic Iconography of the Salpetiere. Massachusetts: Massachusetts Institute of Technology
Josh Ellenbogen (2012). Reasoned and Unreasoned Images: the Photography of Bertillon, Galton, and Marey. Pennsylvania: The Pennsylvania State University Press.
Michel Foucault (1999). Photogenic Painting. London: Black Dog Publishing.
Michel Foucault (2003). Abnormal: Lectures at the College de France 1974-1975, London: Verso.
Michel Foucault (2005).The Birth of the Clinic. London: Routledge.
Michel Foucault (2006a). History of Madness. London: Routledge.
Michel Foucault (2006b). Psychiatric Power: Lectures at the Collège de France, 1973-1974. London and New York: Palgrave Macmillan.
Sander Gilman (1976). The Face of Madness: Hugh W. Diamond and the Origin of Psychiatric Photography. New York: Brunner/Mazel.
Sander Gilman (1982). Seeing the Insane. New York: John Wiley & Sons.
Sander Gilman (1993). ‘The Image of the Hysteric’, in Hysteria Beyond Freud. Berkley and Los Angeles, University of California Press.
Emily Godbey (2000). ‘Picture me Sane: Photography and the Magic Lantern in a Nineteenth-Century Asylum,’ in American Studies, 41:1, 31-69.
David G. Horn (2003). The Criminal Body. Lombroso and the Anatomy of Deviance. New York: Routledge.
David Houston Jones (2005). ‘The Body Eclectic: Viewing Bodily Modification in
David Nebreda.’ In Reconstruction 5.1, Studies in Contemporary Culture.
George S. Layne (1981). ‘Kirkbride-Langenheim Collaboration: Early use of Photography in Psychiatric Treatment in Philadelphia,’ in The Pennsylvania Magazine of History and Biography, Vol 105, No 2, pp. 182-202.
Hugh C. Marles (1992). ;Duchenne de Boulogne: Le Mechanisme de la Physiognomie Humaine.’ History of Photography 16.4: 396.
John Tagg (1988). The Burden of Representation: Essays on Photographies and other Histories. New York: Palgrave MacMillan.
Paul Virilio (1994). The Vision Machine. Indiana: Indiana University Press.